OSSICULOPLASTY
Ossiculoplasty is the reconstruction of the middle ear ossicular chain which has been disrupted or destroyed by the use of interpositioned implants which help in regaining the original mechanics of the ossicular chain to transfer the sound energy to the inner ear.
Ossicular abnormalities can range from loss of ossicular continuity due to trauma, congenital,surgical manipulation or middle ear pathology such as cholesteatoma or fixation of the ossicles in cases of otosclerosis or it can be in combination.
Aetiology of Ossicular abnormalities:
- Cholesteatoma.
- Chronic suppurative otitis media.
- Trauma.
- Congenital malformation
Contraindications for Ossiculoplasty:
- Active infection in the ear is the only true contraindication.
- Relative contraindications include persistent middle ear mucosal disease, sensorineural hearing loss and repeated unsuccessful use of the same or similar prosthesis.
Candidates for Ossiculoplasty:
- The clinical presentation of patients who would benefit from ossiculoplasty is quite variable.
- The goal of ossicular chain reconstruction is better-hearing, most typically for conversational speech.
- The aim of ossiculoplasty is not only to close the air-bone gap but to improve the patient’s overall hearing (improve the air conduction score).
- A patient’s perceived hearing improvement is best when the hearing level of the poorer-hearing ear is raised to a level close to that of the better-hearing ear.
- Small improvements in hearing are more likely to be appreciated by patients with bilateral hearing loss.
- In most cases, the worst ear is selected for surgery, but unless the surgery can restore symmetrical or nearly symmetrical hearing, or convert the operated ear into the better ear, the patient is unlikely to experience a reduction in disability.
- The conductive hearing loss may be the result of ossicular erosion or fixation from chronic ear disease, blunt or penetrating trauma, or congenital or neoplastic causes.
- It may also be associated with inner ear causes. These inner ear causes include superior semicircular canal dehiscence and an enlarged vestibular aqueduct. In these conditions ossiculoplasty is not useful.
Materials used for Ossiculoplasty
- 1. The materials used in ossiculoplasty can be autografts or homografts or of synthetic materials.
- 2. Autografts:
- Includes refashioned ossicles, cortical bone and cartilage.
- They have the advantage of low extrusion rates.
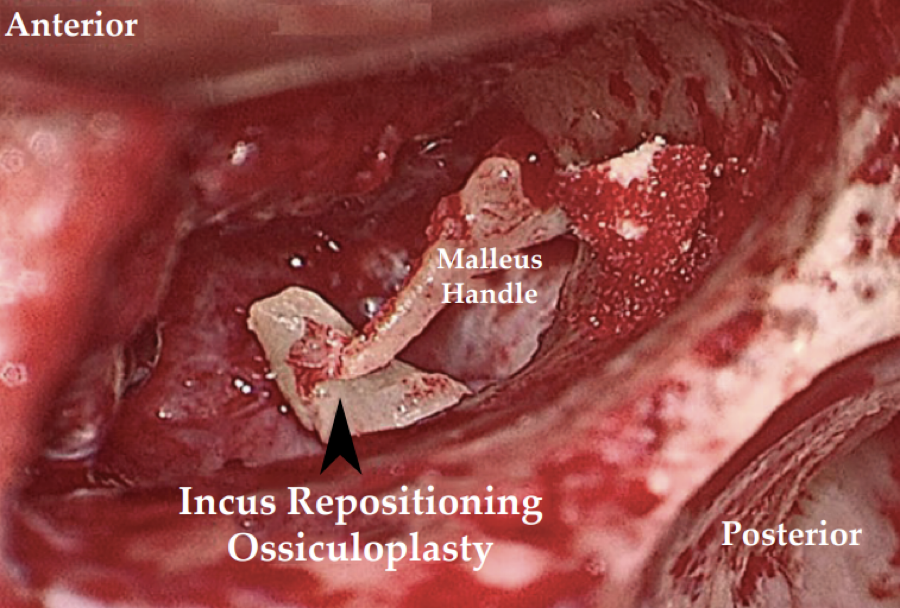
- The most commonly used autograft material has been the incus body, which is often reshaped to fit between the manubrium of the malleus and the stapes capitulum.
- Autograft materials are not always available, or as in patients with cholesteatoma, an ossicle may have microscopic squamous epithelium infiltration that precludes such use.
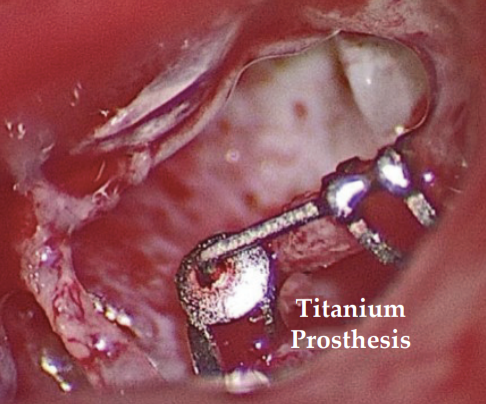
- 3. Alloplastic materials include:
- Metals (titanium and gold)
- Plastics (Plastipore, Proplast, Polyethylenes, Polytetrafluroethylene, or Teflon).
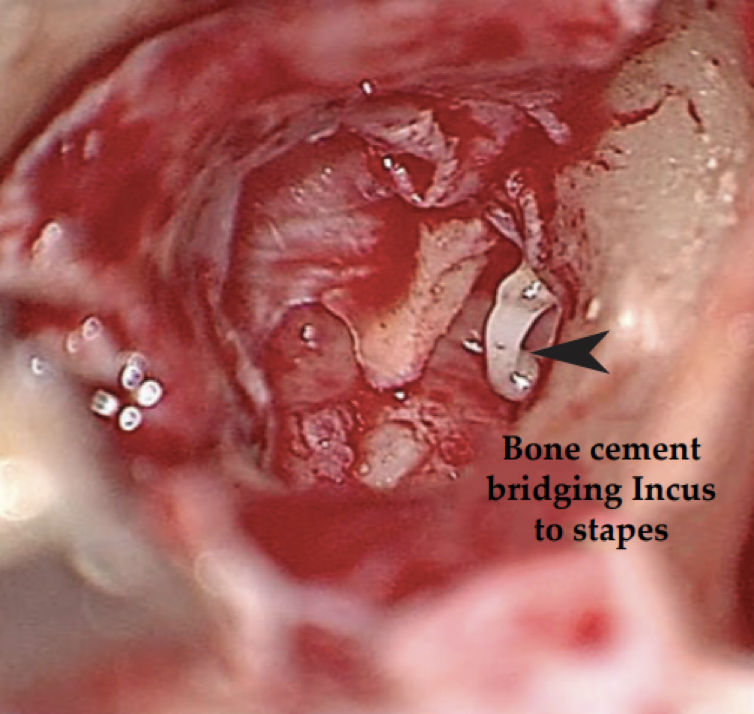
- Biomaterials (Ceramics and Hydroxyapatite)- Bone cement (Glass Ionomer):
- It has good biocompatibility, often used in dental procedures.
- It is very easy to use and much more economical than the prosthesis.
- Bone cement is prepared and shaped easily. After it becomes firm it doesn’t get affected by any fluids like blood.
- Bone cements are substances produced by an acid-base reaction. This means that formulated powder is mixed with a liquid to generate a mixture that hardens through a reaction.
- Polymaleinate glass ionomer cement is a commercially available bone cement that can be used to reconstruct a discontinuity between the ossicular chain - most commonly the incus and the stapes.